// A Tale of Two Manuals
DSM vs. ICD
Both manuals exist to standardize diagnosis. When it comes to complex trauma, they arrived at very different conclusions.
- DSM (U.S.-based): Produced by the American Psychiatric Association. It governs North American diagnosis and insurance billing — which means whatever the DSM recognizes or ignores doesn't just shape academic debate. It shapes whether people get the right treatment.
- ICD (Global): Published by the World Health Organization. It covers all medical and mental health conditions and is used by governments and public health systems worldwide — including, increasingly, by Canadian clinicians working outside strict billing constraints.
How they diverged around trauma:
- Early editions: Both treated PTSD as a response to a single, discrete traumatic event — combat, disaster, assault. There was no framework for trauma that was chronic, relational, or developmental. If your damage accumulated slowly over years, the manuals didn't have a box for you.
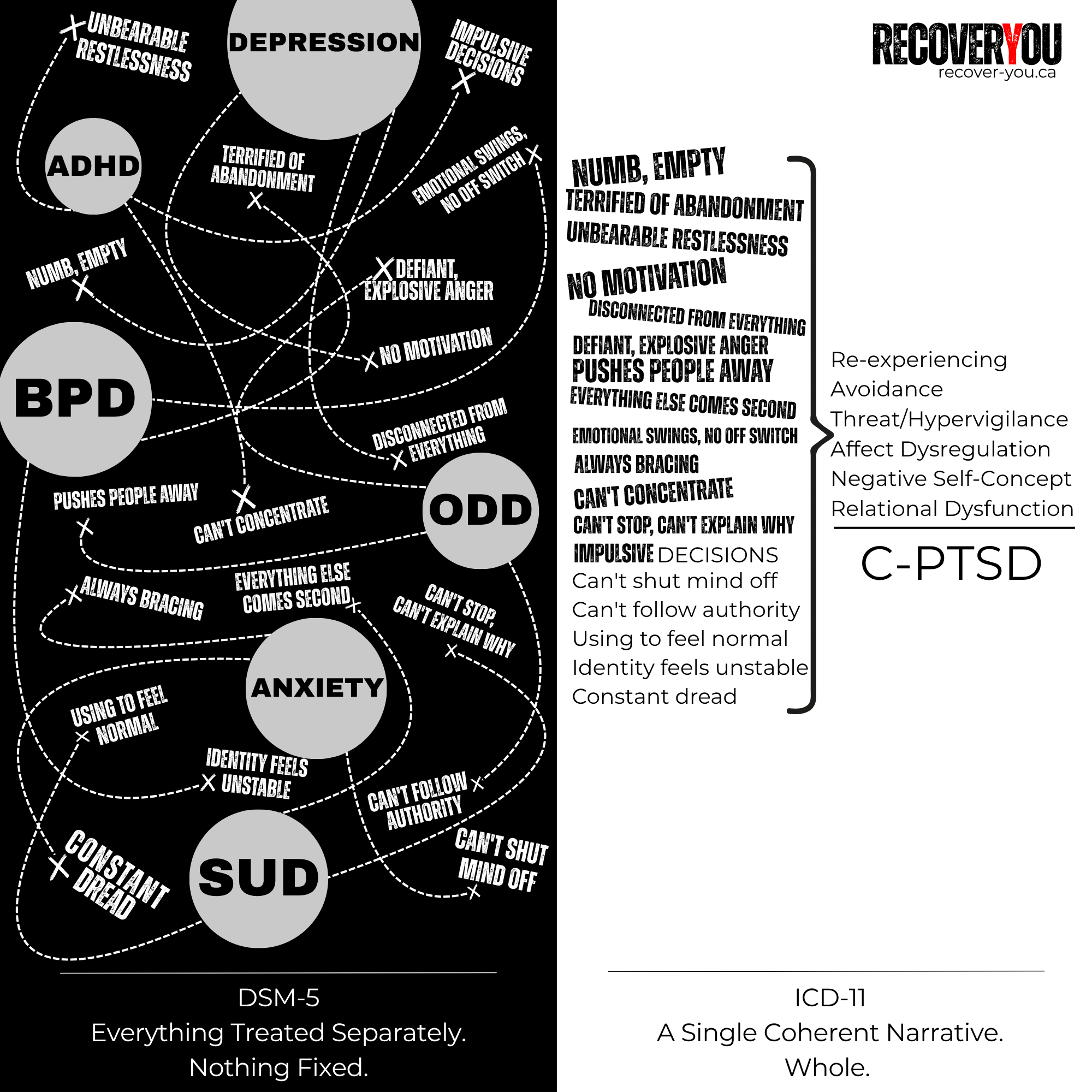
- DSM-5 (2013): Expanded PTSD criteria and added a dissociative subtype — genuine progress. But it still rejected both DESNOS and Developmental Trauma Disorder. In practice, that meant complex-trauma survivors continued collecting multiple separate diagnoses rather than one accurate one. The picture was there. Nobody connected the dots.
- ICD-11 (2022): Formally recognized Complex PTSD (C-PTSD) as its own distinct diagnosis — not a subtype of PTSD, not a personality disorder, but a condition that reflects what long-term, repeated, interpersonal trauma actually does to a person.
The global system caught up to what trauma clinicians and survivors had understood for decades. The North American system is still working on it.