// Why This Model Exists
In recovery spaces, I kept seeing the same pattern.
Nearly everyone I met carried heartbreaking stories about their life in addiction. Hundreds of people, maybe thousands, side by side in active use or standing in the same treatment lines. But underneath, almost without exception, were even more painful accounts of early adversity. The people who insisted they had no trauma almost always opened up later, once they felt safe enough.
And yet the systems built to treat addiction and the science built to heal trauma rarely speak to each other. Most addiction programs in Alberta do a genuine job with stabilization, structure, and community. Many proudly identify as "trauma-informed." But trauma-informed care, as it currently exists, is designed to reduce harm. It is not designed to treat the trauma driving the addiction in the first place.
The system doesn't stop short because anyone is indifferent to suffering. Staff are trained. They work hard. They genuinely try to create environments that don't retraumatize people who are already barely holding together. It stops short because the model was never structurally built to carry people through the later phases of trauma recovery. It was designed to stabilize addiction safely, and it does that. What it doesn't do, what it was never designed to do, is support the full arc of trauma integration that durable recovery actually requires.
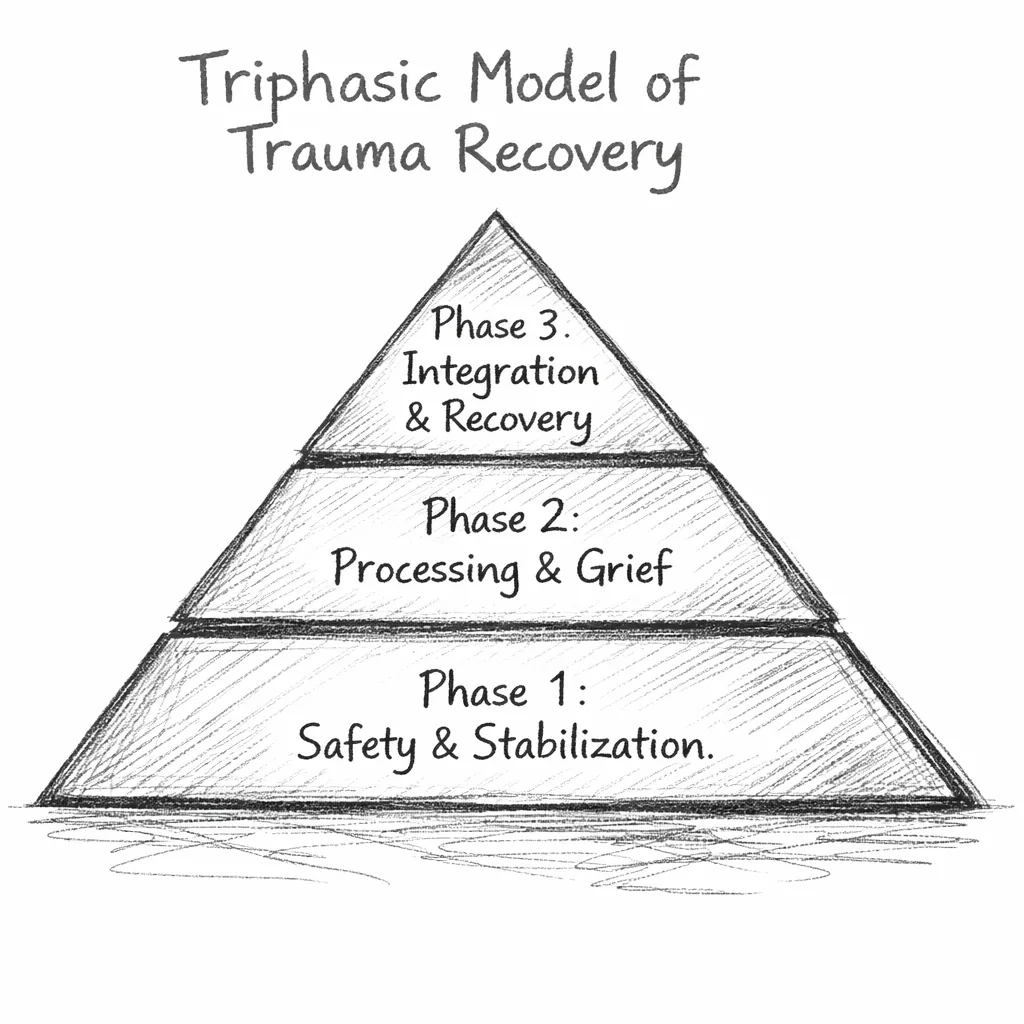
Worth noting: Alberta already draws on Judith Herman's foundational principles of safety, trust, and collaboration. Herman's three-stage framework itself traces back to Pierre Janet, a French psychologist in the 1890s who first proposed that trauma treatment had to be sequenced rather than immediate. In effect, we adopted the opening chapter, establishing safety, and treated it as the whole book.
The result is a system that can stabilize people and prevent immediate harm, but routinely cannot carry them into the deeper, lasting recovery they came looking for.
If we already understand the importance of safety, and we already recognize the central role of trauma, why not build the pathway that actually carries people all the way through?
Less than 5–10% of this material was taught to me in any program I attended. I had to find the rest on my own, and what I found was infinitely more useful than anything the system gave me.
